 |
II./2.4.: Sacral teratoma as the most frequent congenital tumor, and other congenital tumors
II./2.4.1.: Congenital tumors, in general
Tumors developed already at birth, and those developing during the first 3 months of life, are called congenital tumors.
Traditionally, those tumor-like lesions are included in this group which not necessary fulfill the criteria for a real tumor, rather they can be considered choristomas (a node, demarcating from its environment, constituted of regular tissue elements, however, these elements are not typical for the location; e.g. nodes constituting of ectopic breast-, liver-, pancreas tissue), or hamartomas (a node, demarcating from its environment, constituted of regular tissue elements typical for the location, however, the ratio of the elements is abnormal; e.g. breasthamartoma, constituted from epithelial-, connective- and adipose tissue elements, but the dominant hypertrophy of the connective tissue makes it separable from the environment).
|
 |
A part of congenital tumors include typically embryonal histological structure, and thus, they can be called embryonal tumors. The most frequent congenital tumors are different teratomas and the congenital neuroblastoma. These are followed by the different mesenchymal tumors, renal tumors and brain tumors. More rarely observable neonatal tumors are the Langerhan’s cell histiocytosis, the hepatoblastoma, and the retinoblastoma. Congenital leukaemia is rare, as well as lymphomas, in this age group. A part of congenital tumors (e.g. familial Wilms-tumor, cca. 40% of retinoblastomas) are heritable.
Certain heritable syndromes may be associated with congenital tumors, or with tumors manifesting in early childhood (e.g. Type I glycogenosis + hepatocellular carcinoma; lack of alpha-1-antitripsin + hepatocellular carcinoma; type I neurofibromatosis + brain tumors, sarcomas, leukaemia; sclerosis tuberosa + brain tumors; xeroderma pigmentosum + skin cancer, melanoma; Wiskott-Aldrich-syndrome + leukaemia, etc.). In numerous cases, constitutional chromosoma aberrations co-occur with congenital tumors (e.g. Down-syndrome + acute leukaemia; 13q-syndrome + retinoblastoma; trisomy18 + nephroblastoma, etc.).
In sporadically occurring, multiplex developmental disorders, specific tumor types can also be observable (e.g. Beckwith-Wiedemann-syndrome + nephroblastoma, adrenal-carcinoma, hepatoblastoma; Hirschsprung-disease + neuroblastoma). It is because teratogenesis and oncogenesis are closely related. A harmful factor, which induces the development of a tumor in the fetus, or postnatally in newborns, causes developmental disorders if affecting the early stage embryo, and vica versa. For example, dietil-stilboestrol – a substance, applied to avoid threataned abortion up till the end of the ’70-s – administered before the 20th gestational week causes developmental disturbances in the uterus, additionally, in young girls, it leads to the development of the, otherwise rarely occurring, clear cell vagina carcinoma.
II./2.4.2.: Congenital tumors and tumors occurring during infancy
|

Look into the table!
|
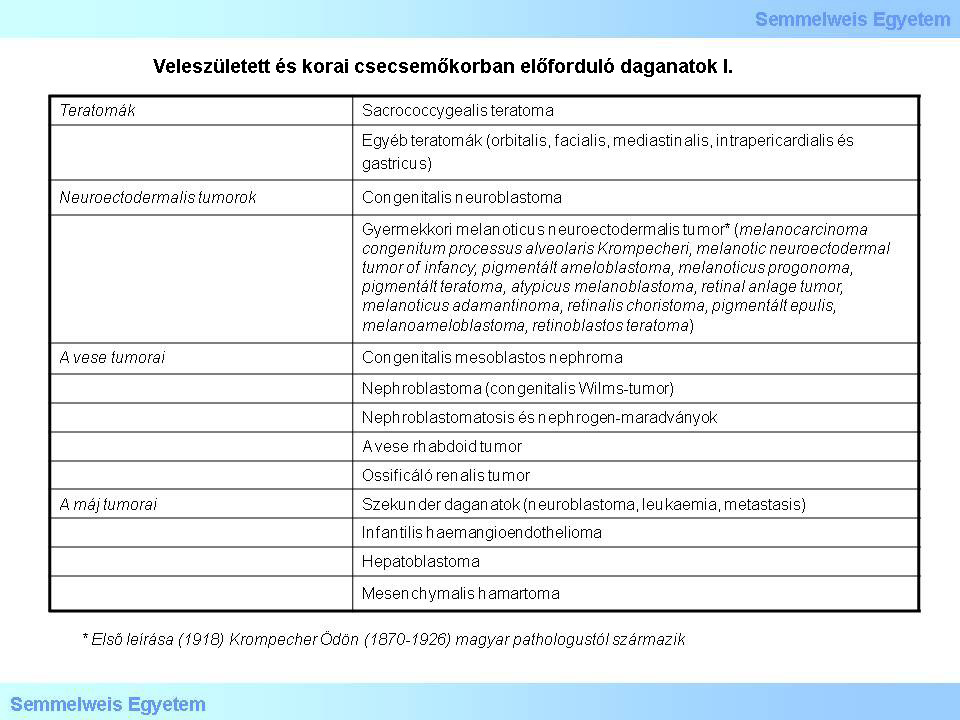
1. table
|
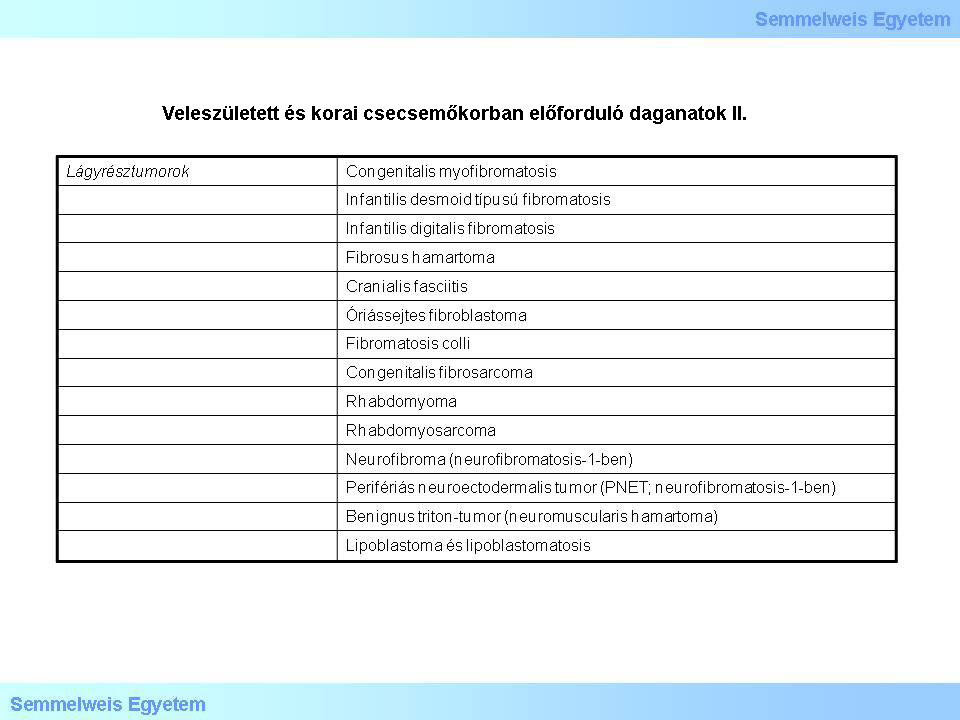
2. table
|
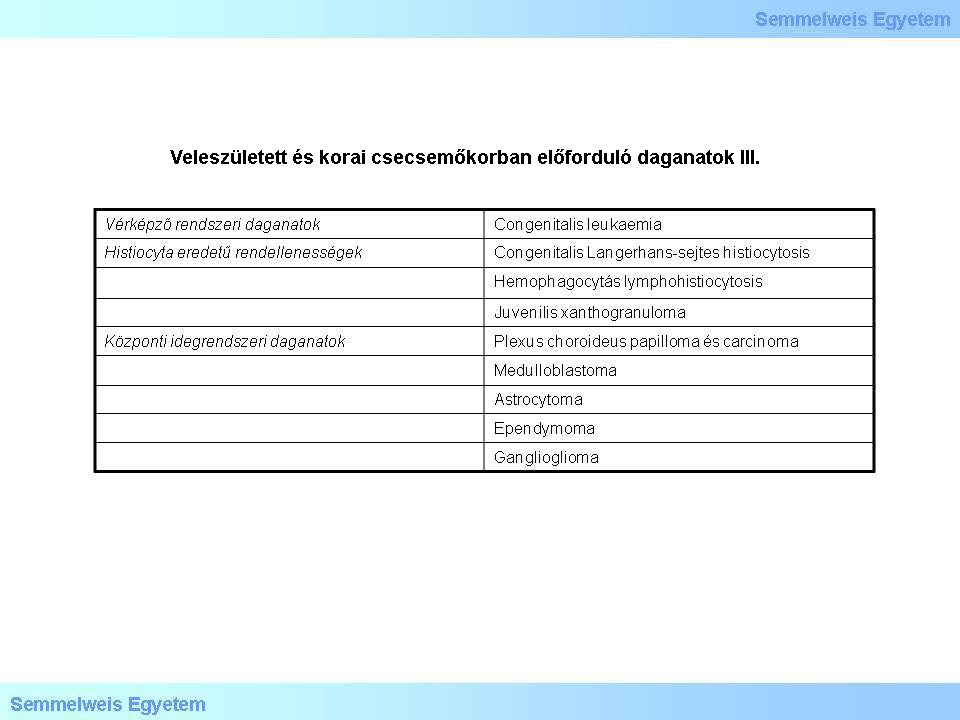
3. table
|
II./2.4.3.: Congenital teratomas
The most frequent congenital tumors are the teratomas, (the so called „miracle tumors”), mainly developing in different levels - most frequently on a sacrococcygeal location - of the midline. They originate from totipotent germ cells, and generally, they contain elements from all three germ layers. It happens, however, that the representation of one of the germ layers is so dominant that the other two layers are not, or hardly represented (so called monodermal teratoma): for instanse, in case of the over-dominance of the ectodermal elements, the cystic tumor is lined only by multilayer squamous epithelium with regular skin appendices – this is called the dermoid cyst –, and in case of over-dominance of endodermal elements, namely thyroid tissue, the so called struma ovarii develops.
Sometimes it is difficult to distinguish teratomas, containing highly differentiated tissue- and organ particules, and the so called „parazite-twin” (foetus in fetu) lesions. The typical difference is that in teratomas the tissue growth is never organized around the notochord or the vertebral axis. The most important prognostic factors of congenital teratomas are the presence (poor), or abscence (good) of the yolk sac tumor, the location of the tumor, and the totality of the excision. It is important to note, that in this age group, the presence of undifferentiated nervous tissue elements is not a sign of malignancy (Micrograph 1)! The ratio of benign vs. malignant congenital teratomas is cca. 40:1.
|
Look into the pictures!
|
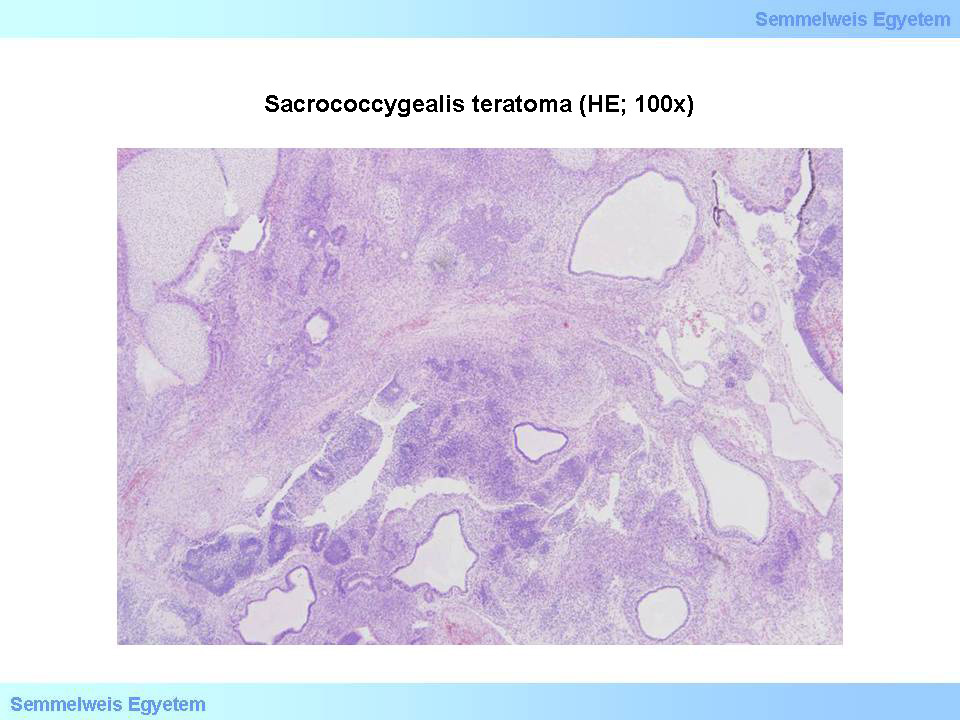
Micrograph 1: Sacrococcygeal teratoma (HE; 100x).Contains differentiated chondroid tissue, cysts lined with a variety of epithelium; neurotubules, undifferentiated neural elements can also be observable within. In the upper right corner, there is a cyst as well, lined with brown-pigmented surface, that can be identified as retinal pigment epithelium (From the archive of the Semmelweis University, 2nd Department of Pathology–collection of Ildikó Szirtes)
|
The most frequent among the congenital teratomas is the sacrococcygeal teratoma, which represents an individual entitiy. It is generally sporadic, but its familiar form is also known, and frequently co-occurs with developmental disorders of the distal intestinal system, the urogenital tract, and the the caudal spinal chord. Already during the second trimester, it can be easily identified with ultrasound, as sacral- or coccygeal protrusion, especially if it causes an elevation of the maternal serum alpha-foetoprotein level too. If the protrusion is too big, it can cause an obstacle during labour. In forms with rich vascularization, complications may occur, such as the development of vascular shunts, bleeding, or fetal cardial decompensation.
Teratomas may be located praesacrally (inside teratoma) and postsacrally (outside teratoma), the former is difficult to diagnose. Macroscopically, they are solid-cystic structures, covered with skin, that is ulcerous in certain parts (Macrographs 2 and 3). Ten-twenty percent of the sacrococcygeal teratomas is malignant, in which yolk sac tumorand embryonal carcinoma particules can also be observed.
|
Look into the pictures!
|
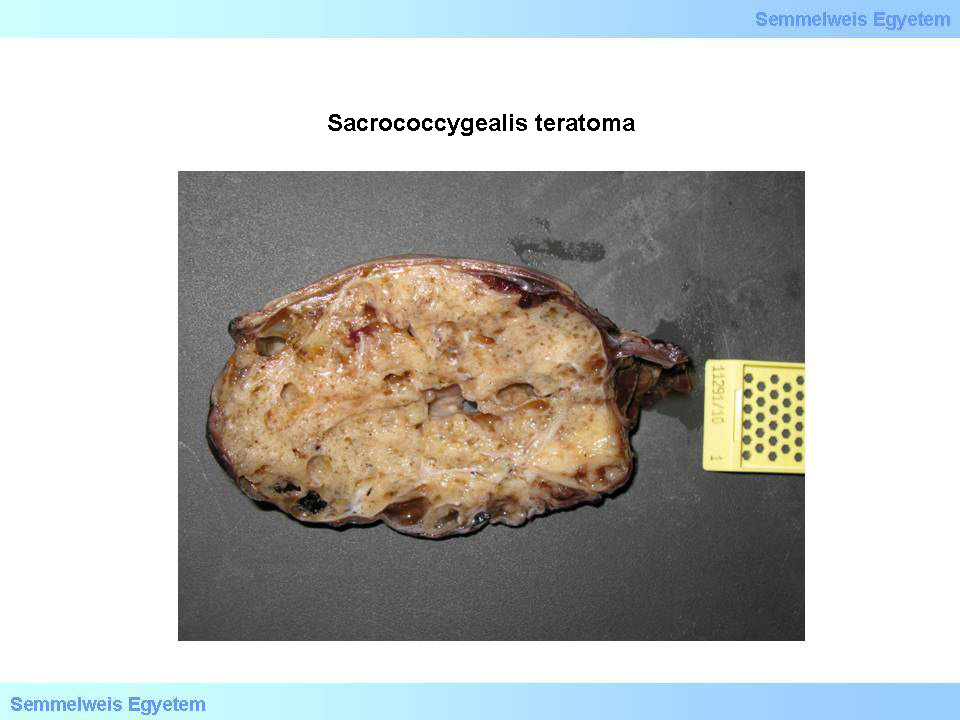
Macrograph 2: Sacrococcygeal teratoma. On the cut-surface of the congenital protrusion, typically solid, in parts, cystically transformed parenchyma can be identified. The macroscopic picture does not refer to the ratio of differentiated and undifferentiated elements, or to direct sign of malignancy, this can only be evaluated by precise pathohistological analysis. (From the image-archive of the Semmelweis University, 2nd Department of Pathology–collection of Attila Kovács and Ildikó Szirtes)
|

Macrograph 3: Sacrococcygeal teratoma. The cut-surface of the tumorous tumescence dominantly shows cystic regions (From the image-archive of the Semmelweis University, 2nd Department of Pathology–collection of Attila Kovács and Ildikó Szirtes)
|
Otherwise, they can include highly differentiated tissue parts (Micrographs 2 and 3). During surgical intervention, the total excision, and the removal of the coccygeal bone are of great importance. Although, in general, the prognosis is good, recurrence may occur.
|
Look into the pictures!
|
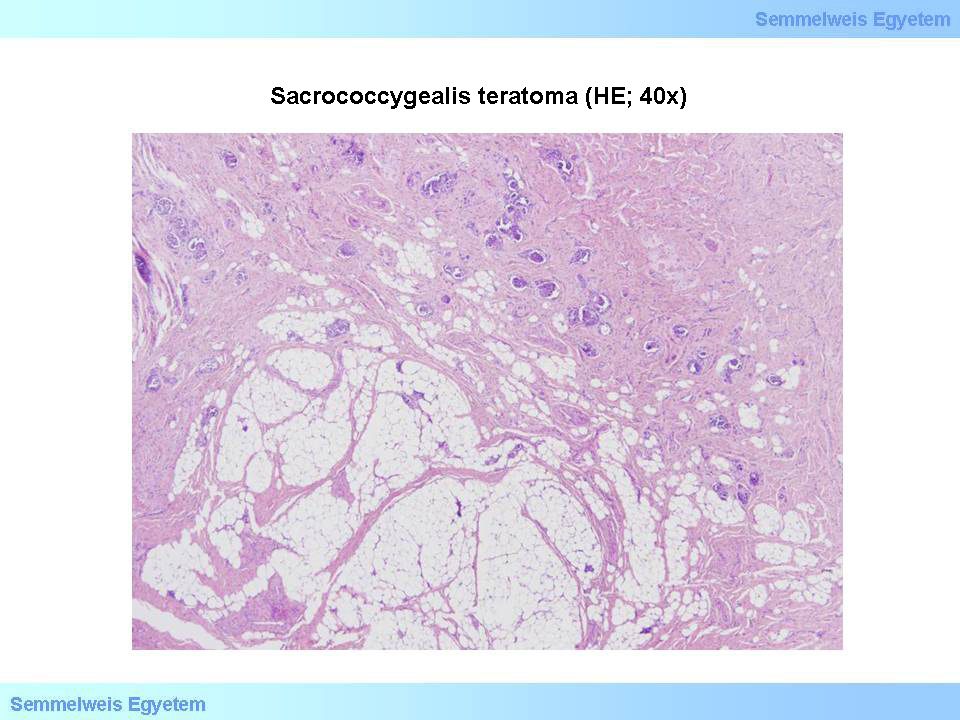
Micrograph 2: Sacrococcygeal teratoma (HE; 40x). Parenchyma, typically constituted of mesodermal tissue can be observed, with differentiated smooth muscule- and adipose tissue, and glomeruloid structures reminding to renal tissue. (From the archive of the Semmelweis University, 2nd Department of Pathology–collection of Ildikó Szirtes)
|
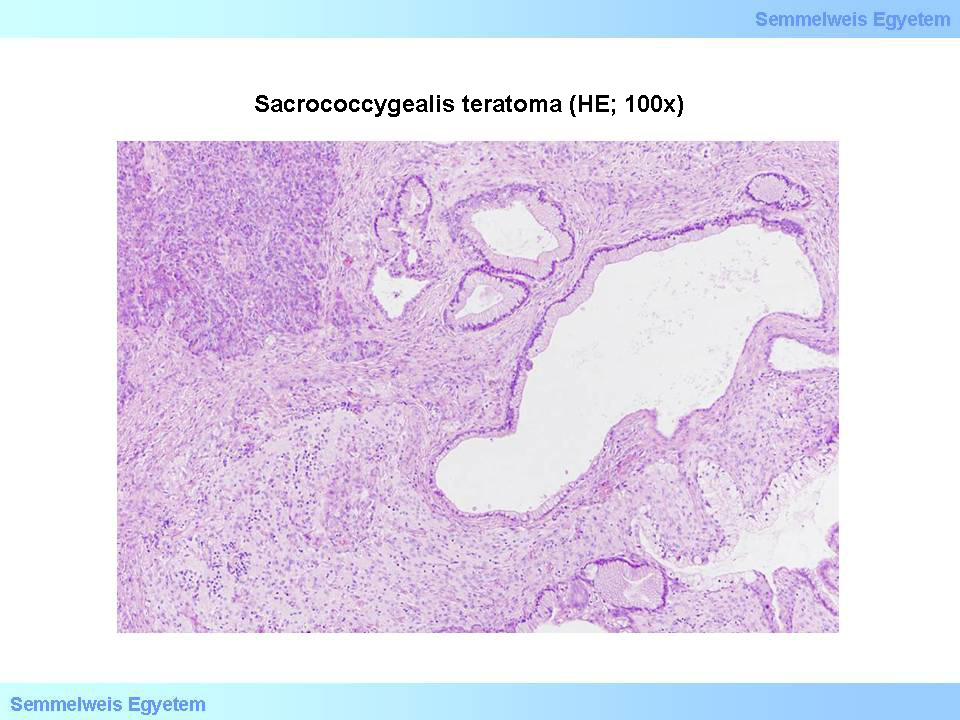
Micrograph 3: Sacrococcygeal teratoma (HE; 100x). Derivates of all three germ layers can be found: ectoderm is represented by mature brain tissue, mesoderm is represented by connective- and smooth muscle tissue, while endoderm is represented by a group of pancreas-like cells. Cysts are lined by differentiated epithelium with various appearance. (From the archive of the Semmelweis University, 2nd Department of Pathology–collection of Ildikó Szirtes)
|
|
|