| |
II/2.6: Rheumatic fever
II/2.6.1: Definition
|
 |
Rheumatic fever is an acute, immunopathogenic, systemic non-purulent inflammation, which is a disease of the whole mesenchymal system of the body, and as such, it belongs to the gorup of so-called collagen diseases.
II/2.6.2: Pathogenesis
Cross reaction against the body’s own structures (connective tissue material) a few weeks after pharyngitis caused by beta-haemolytic Streptococcus A infection
.
II/2.6.3: Typical symptoms
|
 |
Typical symptoms of rheumatic fever include high fever, inflammatory heart disease (carditis), migrating polyarthritis (migrating rheumatic polyarthritis), subcutaneous rheumatic nodes, marginate erythema on the skin, and chorea minor (Sydenham chorea). The most important of all these, influencing the patient’s life expectancies the most is rheumatic heart disease which is a complex disease consisting of valvular endocarditis, rheumatic myocarditis and rheumatic pericarditis. The complete form of heart disease affecting all components of the heart is called rheumatic pancarditis.
II/2.6.4: Rheumatic carditis
II/2.6.4.1: Rheumatic endocarditis
In the acute period valvular oedema is typical which is rich in mucopolysaccharides. Several 1-2 mm, soft, crumbling, reddish, wipeable appositions consisting of aggregated platelets are seen in a string-of-pearls pattern on the closing edge of the valves (macroscopic image No.6). In most of the cases it is followed by complete healing. In some cases however, capillaries grow into the valvular tissue, and this is how the process starts to become chronic, and the appositions begin to organize.
|

Study the image!
|
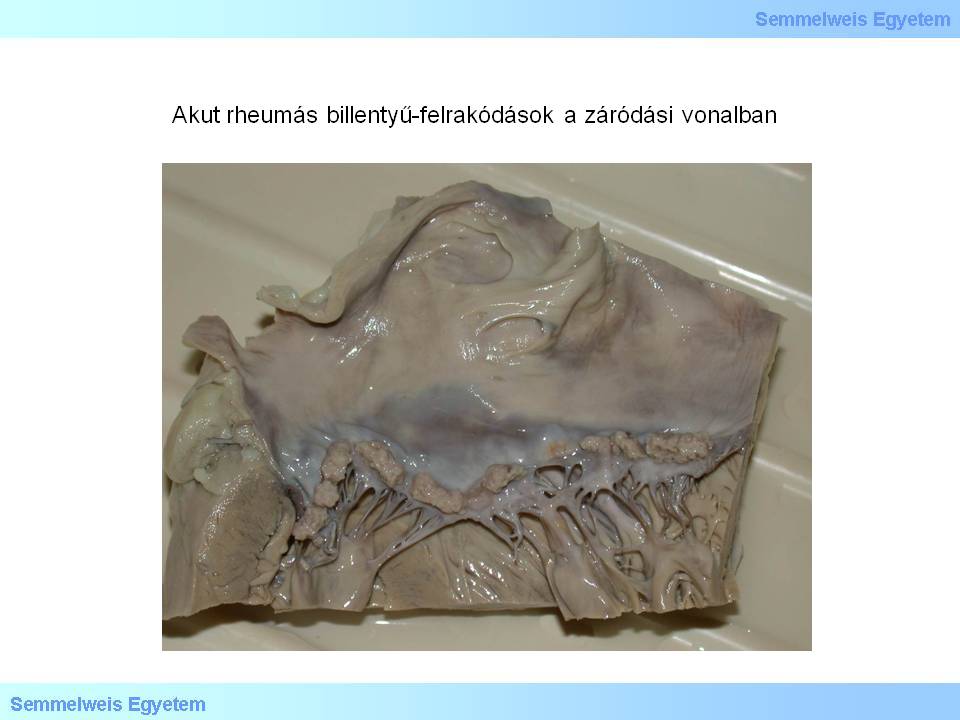
Macroscopic image No.6: Acute rheumatic valvular appositions on the closing edge. (From the collection of the 2nd Institute for Pathology, Semmelweis University – collected by Tibor Glasz).
|
During the transition into chronic form (chronic rheumatic endocarditis) valvular structures get scarred, roughly calcified and thereby morphologically deformed, the cumissurae fuse, and thus starts the rheumatic valvular heart disease. Topographically the most frequently affected valves are the mitral valves (70-75%), less frequently mitral and aortic valves get sick together (25%), and rheumatic lesions in tricuspid and pulmonary valves are very rare. Transition into chronic rheumatic heart disease may last for several years (5-30 years). Probability of chronic heart disease development following the acute period of rheumatic fever is varying between 18 and 65 percents. Rheumatic fever is prone to recurrence, and the cardiac lesions get more severe after each recurrence: recidive or recurrent rheumatic endocarditis. For the same reason, the already existing valvular lesions (e.g. rheumatic or degenerative valvular deformity, congenital bicuspid aortic valve) increase the risk of rheumatic valvular disease or its recurrence.
II/2.6.4.2: Rheumatic myocarditis
|
 |
Also, rheumatic myocarditis can be acute or chronic. Macroscopically, the cut-surface of the myocardium shows barely detectable mottling and small intersitial hemorrhage. Microscopically, rheumatic granulomas (Aschoff bodies) are pathognomonic lesions. These are small perivascular inflammatory foci, consisting of aggregated lymphocytes, macrophages and plasma cells, and fibrinoid necrosis and collagen degeneration might form within them. The specific cells of these granulomas are the so-called Anitschkow histiocytes which have their chromatine substance condensated in the middle of the nucleus, therefore it looks like an owl’s eye.
Another specific cell type is the multinucleated Aschoff giant cell, which is formed by fused Anitschkow histiocytes.
Rheumatic granuloma may also form:
-
- in the pericardium (rheumatic pericarditis), and it becomes scarred when it turns chronic, and
-
- in articular capsules and in soft tissues around the joints, and this is the morphological basis of migrating polyarthritis, and it heals spontaneously.
II/2.6.4.3: The complications of rheumatic carditis
Congestive cardiac failure may develop as an acute complication which can even be lethal. In the acute period, systemic embolisms may form from the valvular appositions. As for chronic complications, valvular heart diseases of the affected valves must be mentioned on the first place, as well as recurrence of the disease on the already deformed valves: recurrent infective endocarditis (acute exacerbations).
II/2.6.5: Clinical components of rheumatic fever
|
|
(i) Subcutaneous rheumatoid nodules are multiple nodules measuring 5-10 mm around the affected joint (e.g. around the elbow or patella), usually on the extensor surface, and they heal spontaneously.
(ii) Chorea minor (Sydenham chorea) is characterized by involuntary-undesigned, convulsive-twitching, jerking limb movements in the large joints (macroscopic image No.7A), with the sterile encephalitis of the extrapyramidal system in the background. It is typical in childhood, somewhat more frequently in girls, and heals spontaneously. The patient’s handwriting indicates the disease’s general condition and changes, therefore it is suitable for monitoring the clinical picture (macroscopic images No.7B-C).
|
Study the images!
|
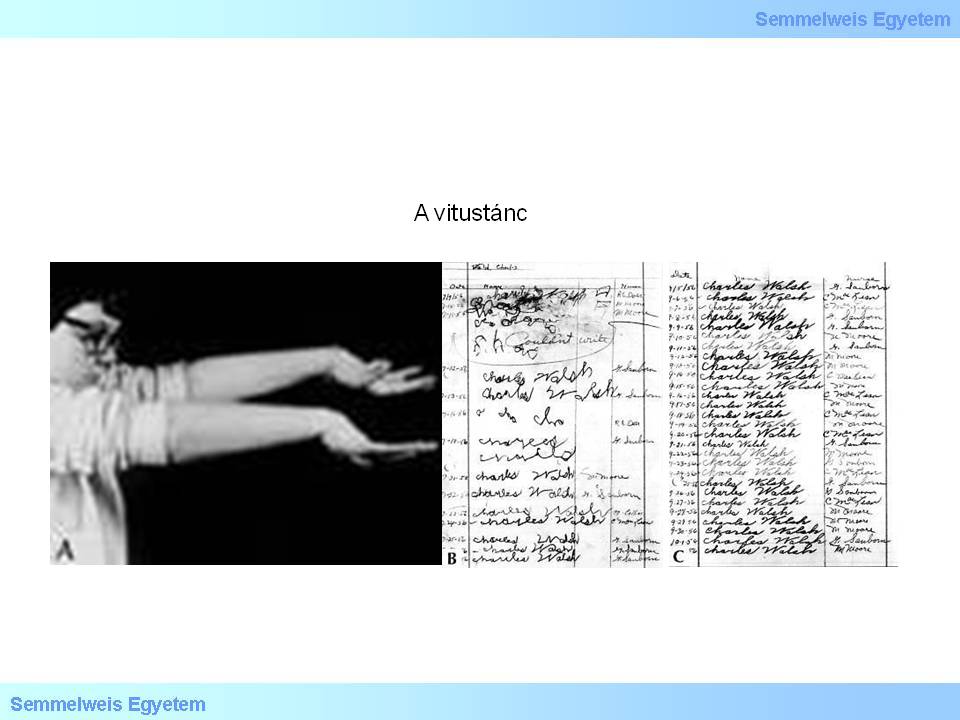
Macroscopic images No.7A-C: A: Sydenham chorea is characterized by convulsive-twitching, innvoluntary-undesigned, jerking movements in the large joints, and I has sterile encephalitis of the extrapyramidal system in the background. B-C: The disease course can be followed by monitoring the patient’s handwriting. Handwriting during the disease (B), and after spontaneous healing (C) (source: http://images.md).
|
|
|