| |
I./2.3.: Horseshoe kidney (rens soleiformis seu arcuatus)
I./2.3.1.: Introduction to renal development
|
 |
The kidney originates from the mesoderma. The thoracic mesonephros develops from the caudal part of the cervical pronephros. The mesonephric duct ends in the cloaca. The ureteric bud develops from the mesonephric duct. From the caudal part of the mesonephros develops the metanephros. The final form of the kidney generates from the mesenchymal cells of the metanephros, the metanephric blastema. The metanephric blastema forms S-shaped tubules by pushing into the ampullary region of the proliferating ureteric bud. Capillary loops, differentiated from angioblasts, protrude into the lower part of the tubules, from which glomeruli develop. The proximal convoluted tubule, the loop of Henle, and the distal convoluted tubule develop from the upper part of the tubule.
The collecting duct system, the calyces, the pelvis and the ureter develop from the ureteric bud. Mesodermal cells change phenotype by transdifferentiation and turn to epithelial cells: they form apical zonae occludentes, and basal membrane. First nephrones appear in the 8th gestational week and their formation lasts untill birth. The functional maturing of the nephrones takes place in the gestational months following their formation, but even goes on in the postnatal life. Polycistin-1 and -2, produced in large amounts in the basal regions of epitehilal cells originating from the uretereic but, promote the binding between the actin of the tubular epithelial cells and the interstitial matrix.
The binding anchors the tubules and provides possibility to the formation of the complex spacial structure of tubules and the interstitium. Renal epithelial cells do not forget their mesodermal origin, in the cytosceleton of podocytes there is always vimentin, which is characteristic to mesencymal cells, as well, as vimentin is also detectable transiently in regenerating epithelial cells of the tubules. Moreover, renal cell carcinoma cells show vimentin- and epithelial membrane antigen (EMA-) positivity.
I./2.3.2.: Horseshoe kidney (ren soleiformis seu arcuatus)
|
 |
It develops due to the incomplete separation of the metanephrogenic mass of cells. Its incidence is: 1/1000 urology patients. The two kidneys fuse together at their lower (Figure 1), less frequently, at their upper pole, by either a thin connective tissue-, or a thicker parenchymal bridge (isthmus), at the level of the 4th and 5th vertebrae. Due to the fusion, the developmental migration of the kidneys and the final turn into their position remain incomplete and thus, these kidneys are usually in a lower position than usual, in the lumbar region. The pelvises and calyces face to the front, and the ureters run in front of the kidneys downward to the bladder.
|

Have a look at the image / figure!!
|
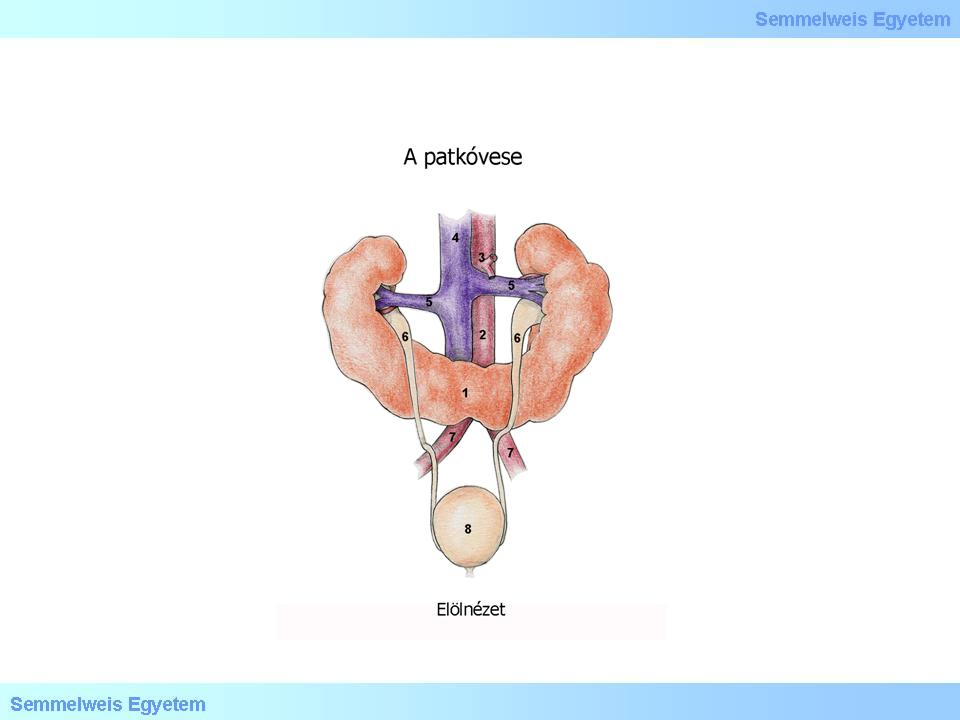
Illustration 1: Horseshoe: (1) Isthmus, (2) Aorta, (3) Arteria mesenterica superior, (4) Vena cava inferior, (5) Venae renales, (6) Ureter, (7) Arteria iliaca communis, (8) Vesica urinaria, (9) Elölnézet.
|
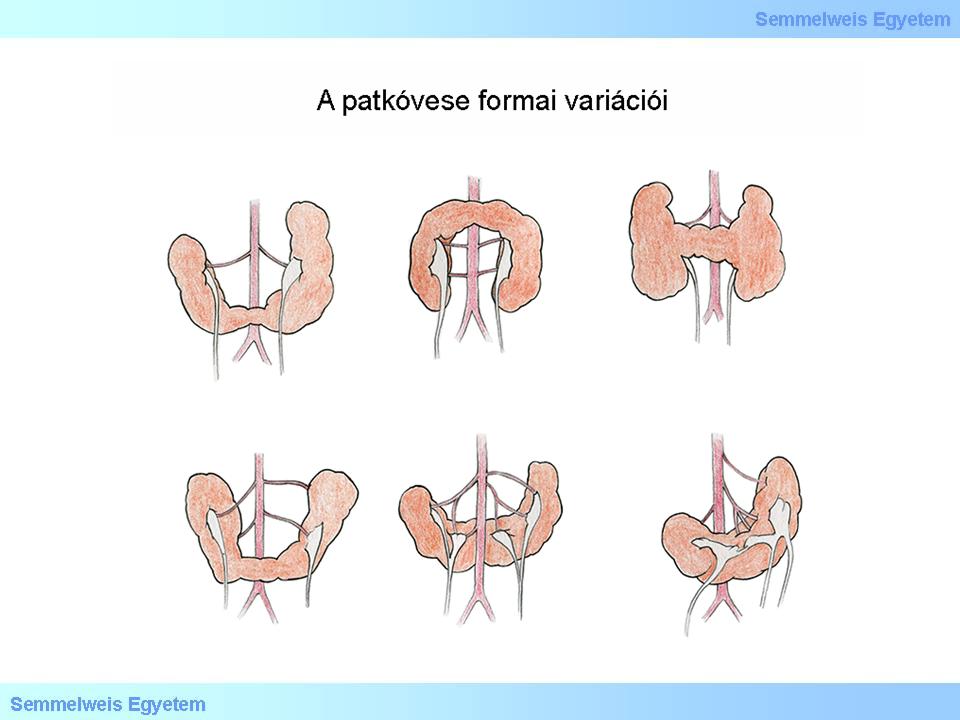
Illustration 2.: A patkóvese formai variációi
|
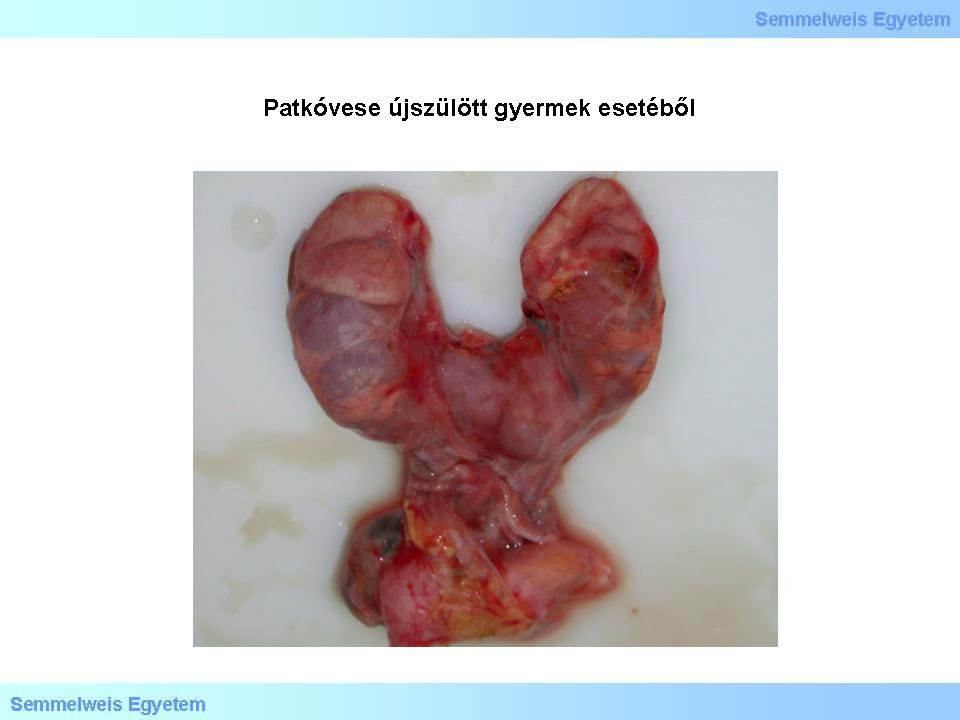
Figure 1: Horseshoe from a case of a newborn. The kidneys fused together by their lower pole and their ureters connecting irregularly to the urinary bladder may cause functional impairments. (From the image-archive of the Semmelweis University, 2nd Department of Pathology–collection of Attila Kovács and Ildikó Szirtes)
|
Due to the position of the kidneys and the deformities of their cavity system, affected subjects are vulnerable to pyelonephritis, and in less severe cases, symptoms include pelvic, lumbar pain, dependent on the posture (starting or increasing when leaning forward or backward), and it typically diminishes when laying. Further complications include kidney stones, in severe cases, hydronephros , pyuria, hematuria, as well, as, according to certain data, increased prevalence for renal malignomas, for example renal cell carcinoma, and transitional cell cancer of the renal pelvis (carcinoma urotheliale seu transitiocellulare pelvis renalis).
|
|
On urography images, the unusual axes of the kidneys draws the attention to this anomaly: The axes of the kidneys converge in cranio-caudal direction. The simplest way of kidney imaging today is ultrasound. If horseshoe kidney does not cause clinical complaints, there is no need for therapeutic intervention, only regular urological (urographic) follow-up. In case of complaints, however intervention is needed: the separation of the kidneys and the correction of their anatomical relations is only possible with operation. The separation of the kidneys usually meets the expectations, complaints diminish. In 25% of horseshoe kidneys, stasis of the cavity system, kidney stone, hydro- or pyonephros occur, and requires therapeutic intervention.
|
|