 |
III/2.1: Main data of the presented specimen case
|
Patient’s age:
|
1 month
|
|
Patient’s sex:
|
male
|
|
Baseline pathological disease:
|
Total transposition of the right and left arterial trunks
|
|
Pathological complication:
|
Subaortic and subpulmonary defect of the interventricular septum
|
|
Pathological complication:
|
Accessory septal ventricle: triventricular and biatrial heart
|
|
Pathological cause of death:
|
Chronic cardiac decompensation
|
|
Pathological accompanying disease:
|
Congenital esophagotracheal fistulas
|
|
Pathological accompanying condition:
|
Status post resection of congenital esophagotracheal fistulas
|
III/2.2: Description of the specimen
III/2.2.1: General description
The specimen belongs to a newborn and displays the heart, the perihilar regions of both lungs, the trachea, and the esophagus as a complex.
III/2.2.2: Description of the heart of a pathological point of view
|
 |
The heart has 4+1 chambers, and has a normal outer appearance and size except that the great arterial trunks are transposed (complete transposition of the great vessels). The position, size, and structure of the right atrium are regular, and the inferior and superior vena cava enter it. The foramen ovale is patent/closed??, ??? mm. The tricuspid valve is intact. The right ventricle is the largest chamber of the heart, its wall width is ??? mm, the trabecular and papillary muscles of its interior relief are bulky, its outflow tract is not narrowed, and it continues in the aorta following regular semilunar valves. The aorta is connected with the pulmonary trunk by a narrow ductus Botalli at around the middle of its arch (macroscopic image 5P-1).
The position, size, and structure of the left atrium are also regular, and the pulmonary veins enter it. The structure of the mitral valve is normal. The left ventricle is somewhat smaller that the right one, its wall thickness is ??? mm, its outflow tract is missing in total, and the ventricular septum inserts at the anteriomedial cusp of the mitral valve. There is a sub-aortic round aperture (septal defect) posteriorly in the upper third of the ventricular septum corresponding the membranaceous part of the septum, and it provides a connection between the left and right ventricle.
Embedded in the thickened muscular middle part of the ventricular septum is an accessory cavity of ??? mm longitudinal and ??? mm horizontal diameter, with partially trabeculated interior surface lined with smooth endocardium which cranially continues into the pulmonary trunk after regular semilunar valves and its caudal end is ??? mm from the apex. Anteriorly on the right lateral wall of this cavity an oval sub-pulmonary septal defect of ??? mm diameter connects the right ventricle and this accessory cavity. The size of the defect is comparable with the cross section of the pulmonary trunk, that is, in a hemodynamical aspect it doesn’t cause any stenosis – at least not in the age displayed by the specimen.
|
 |

1-2. fotó: (1) DORV_1 - komplett TGA, kettős VSD és egy kis accessorius septalis üregből induló TP elölnézet; (2) DORV_2 - komplett TGA, kettős VSD és egy kis accessorius septalis üregből induló TP oldalnézet
|

3. fotó: DORV_3 - komplett TGA, kettős VSD és egy kis accessorius septalis üregből induló TP nézet a bal kamra felöl
|
The pulmonary trunk furcates into regular left and right pulmonary arteries and runs toward the pulmonary parenchyma on both sides. The heart itself has actually five ventricles with two anatomical atria and three ventricles; the odd cavity is considered as an accessory, or tertiary, or septal ventricle.
|
|
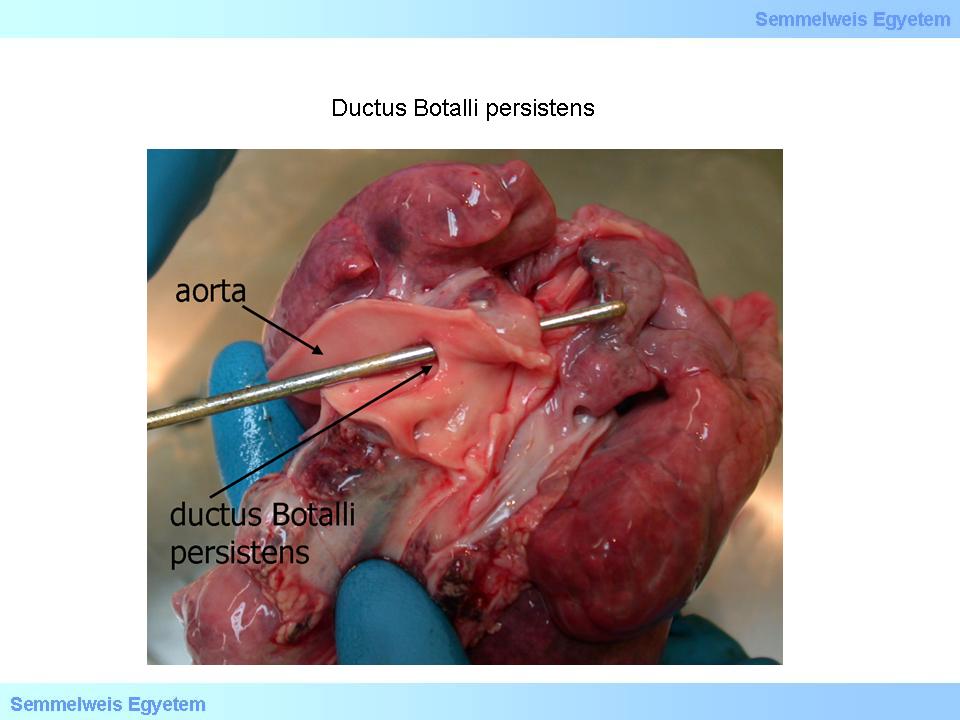
Patent ductus arteriosus. The probe is in the patent ductus Botalli. The duct is an important participant of fetal circulation because the blood that flows through it warrants the fetus’ life within the womb. However, circulatory conditions rearrange after birth in such way that the ductus arteriosus remaining patent will cause harm due to blending of the arterial and venous blood and thus loss of peripheral oxygenation efficacy. Permanent postnatal patency (persistent ductus Botalli) is therefore considered as a pathological condition. (From the archives of the 2nd Institute for Pathology, Semmelweis University – collected by Attila Kovács and István Kenessey).
|
III/2.2.3: Description of the heart of a circulatory point of view
|
|
Under the above described structural circumstances, the bloodflow pathway in the heart was as follows: the blood returning from the body entered the right atrium via the superior and inferior vena cava which were in normal position, and from here it flowed to the right ventricle and through the sub-pulmonary septal defect and the accessory heart chamber to get into the pulmonary trunk and pulmonary circulation. From here the pulmonary veins – which were in regular position – carried the blood back to the left atrium, and it continued its way into the left ventricle, and through the sub-aortic septal defect into the right ventricle and the aorta. So the two circulations crossed each other at the level of the right ventricle, the blood got blended here, and in the same time, the right ventricle had two functional outflow tracts since both transposed great arterial trunks originated from it – the aorta directly and the pulmonary trunk indirectly through the accessory ventricle. The status described here is actually a specific case of double-outlet right ventricle (DORV).
III/2.2.4: Patological description of the trachea and esophagus
The mucous membrane of the trachea is intact, and at the border of the lower and middle third there is a 4 mm longitudinal oval area of bloody discoloration with sharp outline and retracted middle part. On the same level of the esophagus there is a horizontal surgical suture in the full width of the esophagus, the stitches hold well and their environment is peaceful. (Status post surgical closure of esophago-tracheal fistula.)
|
|