| |
III/2.3: Double-outlet right ventricle – DORV
|
 |
The theory of conotruncal malseptation explaining the development of double-outlet right ventricle (DORV) was described by Lev et al in 1972. According to this theory DORV encompasses a whole spectrum of morphological disorders from ventricular septal defect (VSD) presenting with overriding aorta with or without pulmonary stenosis, to Taussig-Bing anomaly and complete transposition of great arteries (TGA) complicated with VSD. Some authors use the diagnosis of DORV only when the great arteries originate from the right ventricle by at least 50% of their cross sections. DORV may develop within the confines of atrial or atrioventricular transition disorders.
One of the main factors that determine the hemodynamic conditions in DORV is the topoanatomical location of VSD which may be:
-
a) sub-aortic,
-
b) sub-pulmonary,
-
c) doubly-committed – similarly close to both great arterial trunks or
-
d) non-committed – similarly far from both great arterial trunks (Drawing No.1).
|

Study the drawings!
|
Caption: Drawing No.1: Possible basic locations of ventricular septal defect: (a) sub-aortic, (b) sub-pulmonary, (c) doubly-committed – similarly close to both great arterial trunks or (d) non-committed – similarly far from both great arterial trunks Source: Surgery for Congenital Heart Defects. Third Edition. Editors Stark JF, de Leval MR, Tsang VT. John Wiley & Sons, Ltd; London 2006; pp. 435.
Sub-aortic VSD is seen in DORV presenting as tetralogy of Fallot, while VSD is sub-pulmonary in the so-called Taussig-Bing anomaly which has similar pathophysiology to that of TGA complicated with VSD. The nomenclature that describes VSD location is sometimes misleading, therefore it is fortunate to use ’sub-aortic’ and ’sub-pulmonary’ only in case of hearts where the relevant arterial trunk overrides on top of the trabecular septum. If both the aorta and the pulmonary trunk originates solely from the right ventricle, and the origin of both great arteries is surrounded by a muscular ring (’double cone’ or ’bilateral funnel’) then VSD should be described as non-committed even if it is located closer to one of the great arteries.
|
 |
On the whole, DORV is a concept which is only useful and plausible if all details of the variable morphology are specified in the actual patient. DORV is often complicated by further malformations, such as any atrioventricular valve deficiency, lack or hypoplasia of any of the ventricles, atrioventricular septal defect (macroscopic image No.2), developmental defect of the pulmonary vessels (so-called total anomalous pulmonary venous connection [TAPVC], where pulmonary veins erraticly insert the right atrium instead of the left, and a widely patent foramen ovale (macroscopic image No.3) or atrial septal defect warrants the child to stay alive with the help of the right-to-left shunt that develops here).
|
Study the image!
|
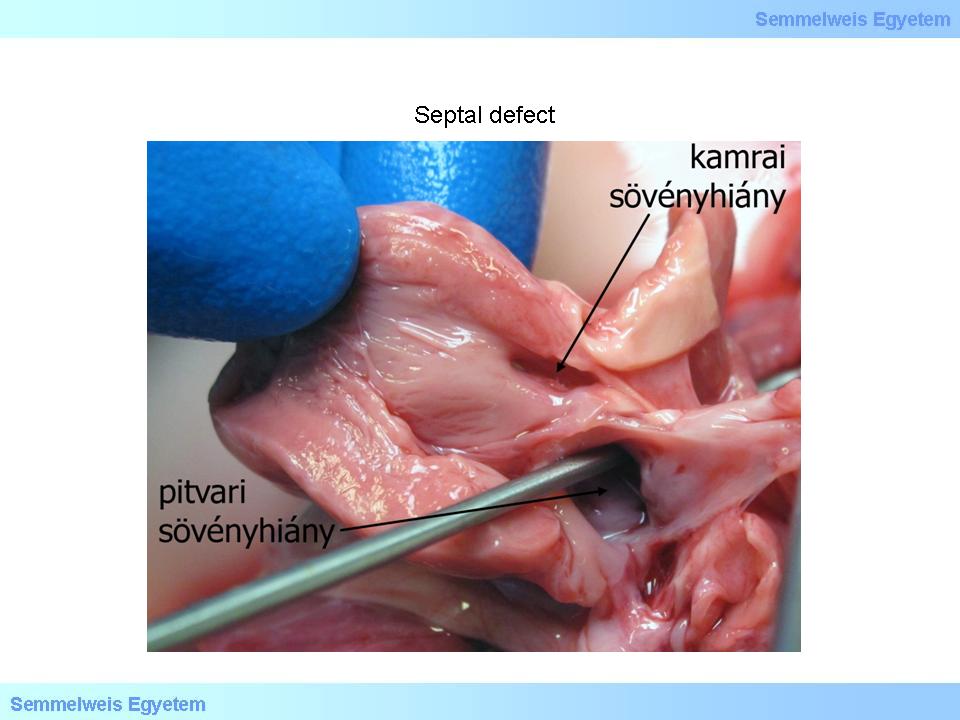
Caption: macroscopic image No.2: Interatrial and interventricular septal defect (atrial septal defect – ASD; ventricular septal defect – VSD). Atrial and ventricular septal defects may range in size, shape, and position from insignificant to life threatening, and they may occur as components of various pathologies and syndromes or independently, alone. (From the archives of the 2nd Institute for Pathology, Semmelweis University – collected by Attila Kovács and István Kenessey).
|
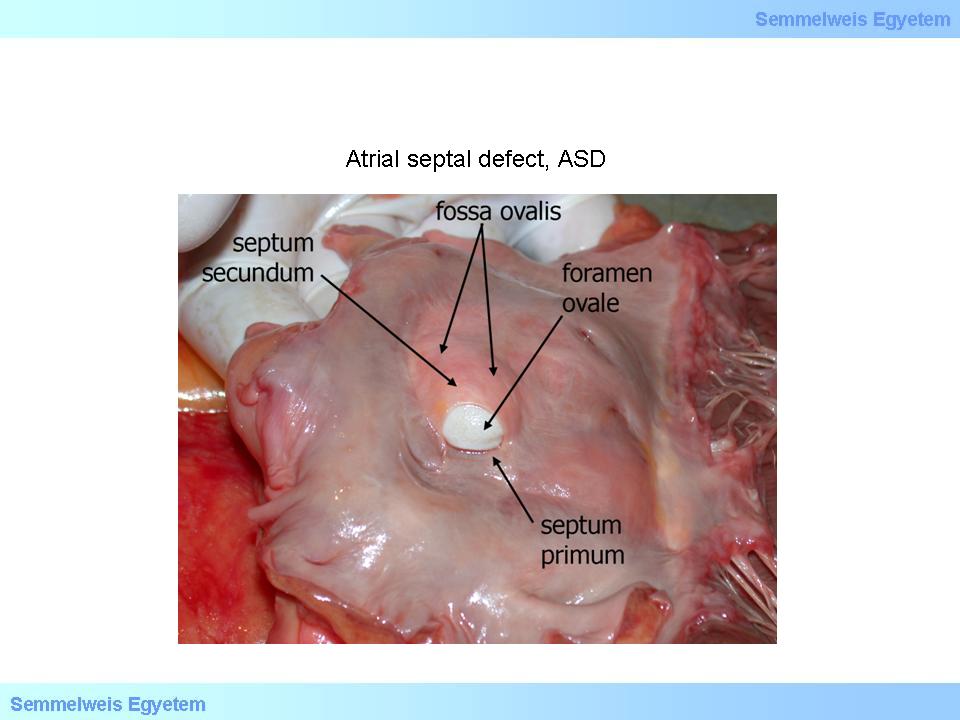
Caption: macroscopic image No.3: Patent foramen ovale. Patent foramen ovale is a part of the fetal circulation but – like the ductus Botalli – it is not needed anymore after birth, therefore normally its two septa – the septum primum and secundum – overlap due to altered pressure conditions, and later they fuse, thus the foramen ovale diappears, and only an oval recess (fossa ovalis) marks its site. When the foramen ovale remains patent after birth it leads to intracardial blending of arterial and venous blood. (From the archives of the 2nd Institute for Pathology, Semmelweis University – collected by Attila Kovács and István Kenessey).
|
Approximately one-third of these cumulated malformations can’t be helped by surgery, intracardial surgery improves the symptoms in another one-third of them, and a further one-third need extracardial valved conduit surgery. The most important factors in the determination of operability are the size of the VSD and its relation to the great arterial trunks and the tricuspid valve, the spatial localization of the two great arterial trunks, the presence or absence of pulmonary valvular or subvalvular stenosis, and the relations of the atrioventricular valves (overriding). The counterpart of DORV (double-outlet left ventricle – DOLV) is very rare. In DOLV both great arterial trunks originate from the left ventricle, by at least 50% of their cross section, too. Accompanying heart malformations include VSD (usually sub-aortic), pulmonary stenosis, Ebstein’s malformation of the tricuspid valve, and hypoplastic right ventricle. This malformation was observed both in situs solitus and situs inversus and in atrioventricular discordance.
|
|