 |
III./3.: Complex congenital heart defect – DORV
Attila Tóth
III./3.1.: Introduction
Double outlet right ventricle (DORV) belongs to the conotruncal heart defects. First descriptions, whose fabricants have already known this abnormality, date back to 1793 and 1893. DORV was specified in 1952 by Branu and colleagues. The expression ’double outlet’ is assigned to AA Calhoun Witham by some authors.
DORV is a heterogeneous abnormality, which can befall independently or as part of other complex congenital heart defects. Several subtypes can be specified which are distinct in clinical manifestation – if present – based on the location of ventricular septal defect (VSD) and the presence of transposition of the great vessels. Similar pressure features of both ventricles are characteristic for this abnormality. Outflow of the morphological left ventricle can be fulfilled towards the morphological right ventricle via the VSD. Without reconstruction, the right ventricle will be hypertrophied due to its „contest” against the systemic pressure. Interpretability of Eisenmenger syndrome is impossible in this constellation. Subpulmonary stenosis is a frequent accessory abnormality which can be even helpful in untreated cases (5R-1. imaging figure) regarding the pulmonary pressure affairs. Namely, pressure gradient, which develops because of the stenosis, decreases the pressure vested for lung, which softens the development of pulmonary hypertension.
|
 |
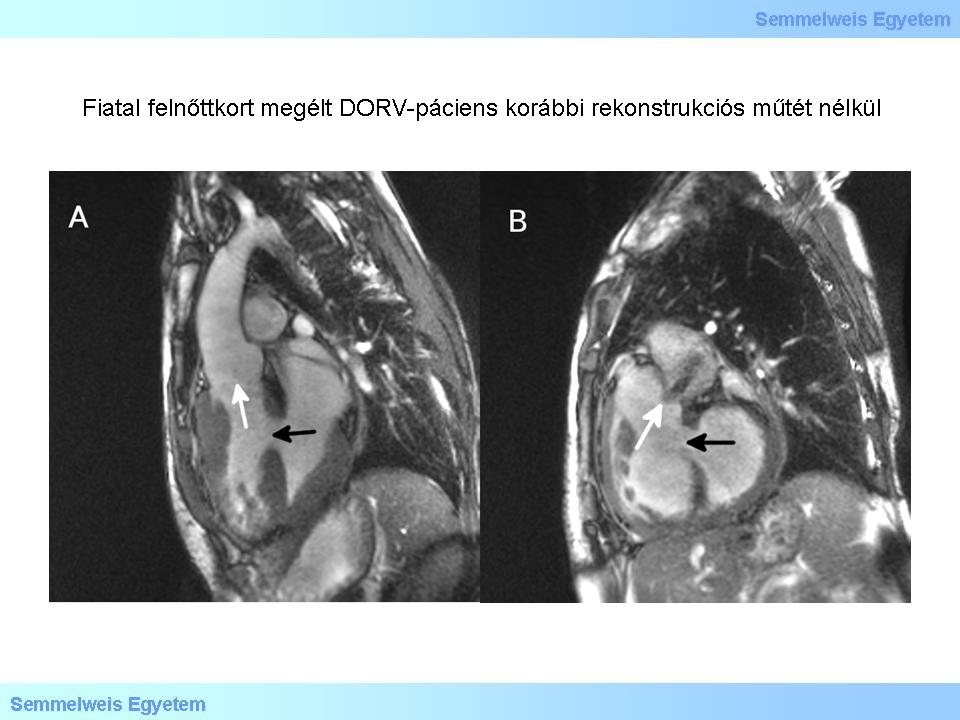
Figure 1.: Patient with DORV who lived until young adulthood without any previous reconstruction surgery. A: Aortic root. Black arrow – VSD; white arrow – aortic root from the morphological right ventricle. B: Pulmonary root. Black arrow – VSD; white arrow – pulmonary root from the morphological right ventricle and the anterograde jet indicating a stenosis.
|
DORV is a relatively rare congenital heart defect. Its incidence accounts for 0,033-0,145 per 1000 live newborn births according to various surveys. VSD and pulmonary stenosis often accompanies with atrioventricular valve abnormalities, right ventricular outflow tract (RVOT) stenosis and obstructive anomalies of the aortic arch. Less frequently accompanying abnormalities include antrioventricular septum defect (AVSD), juxtaposition of the left auricula, superoinferior ventricles, crossed atrioventricular connections, congenital defects of systemic or pulmonary venous backflow, or hypoplasia of any ventricle.
In case of such DORV, where VSD is situated in subpulmonary location besides the transposition of great vessels, Taussig-Bing-anomaly (5R-2. imaging figure) title is used. (Helen B. Taussig and Richard J. Bing played important roles in the elaboration and development of the treatment of congenital heart defects.) RVOT-obstruction is often accompanied with abnormalities of atrioventricular valves and coarctation. If the two-chamber reconstruction is feasible, the term „Rastelli type procedure” is used. In the course of this surgery, blood gets over the previous VSD from the left ventricle in the aorta with a deflector spot, and pulmonary artery is substituted by a homograft. Homograft is a preserved piece of vessel of human origin, which is chosen for the patient in a tissue bank operated in a specialized institution.

Figure 2.: Taussig-Bing-anomaly following Rastelli-type surgery. A: Reconstructed left ventricle outflow. White arrow – blood flow through VSD in the aorta along the deflector spot; black arrow – deflector spot. B: Homograft starting from the right ventricular outflow. Thick black arrow – homograft valve stenosis is indicated by anterograde jet formation; thin black arrow – deflector spot; thick white arrow – remnant of original pulmonary artery (not functioning any more); thin white arrow – section of the aorta’s origin. C: Roots. Thick white arrow – section of the homograft’s origin; thick black arrow – aortic valve with three cusps; thin black arrow – bicuspid pulmonary valve (not functioning any more). D: Gerbode type shunt. Black arrow – Gerbode-jet.
|
The chapter structure
|
|
-
-
III./3.2.: Imaging modalities in DORV
-
References
|
 |
Freedom RM et al: The Natural and Modified History of Congenital Heart Disease. 19A: The Divided Right Ventricle. Wiley-Blackwell, 2006, pp. 232-235.
Freedom RM et al: The Natural and Modified History of Congenital Heart Disease, 28: Double-Outlet Ventricle. Wiley-Blackwell, 2006, pp. 370-380.
|
|